By: Brian A. Hemstreet, PharmD, FCCP, BCPS

http://www.ucdenver.edu/academics/colleges/pharmacy/Departments/ClinicalPharmacy/DOCPFaculty/H-P/Pages/Brian-Hemstreet,-PharmD.aspx
These relationships between the refrac Incomitant and Comitant Squint tive condition and path of the squint are hiv infection detection period discount rebetol 200 mg on line, nevertheless jiangmin antivirus guard generic rebetol 200mg fast delivery, by Incomitant no means invariable hiv infection rates global order rebetol 200 mg overnight delivery. Squint (Paralytic Comitant If the fusion mechanism is properly-developed and the Clinical Features or Restrictive) Squint deviation slight anti viral pharyngitis buy rebetol american express, visible alignment could also be maintained in regular circumstances by a continued effort of fusion: the Magnitude of squint Varies with eye Same in all place positions squint is then latent and might solely be made manifest * when fusion is made impossible (as by covering one eye). Diplopia Usually current Usually absent this condition is called heterophoria or latent squint. If, Ocular movements Restricted Full on the other hand, the upkeep of alignment becomes False projection Present Absent impossible, a real or manifest comitant squint develops. Comitant strabismus could also be intermittent (periodic) or Abnormal head Usually current Absent constant, convergent or divergent. It could turn into manifest after an attack of whooping cough, measles or other debilitating sickness, and is commonly popularly attributed to some such cause. Congenital esotropia can also be associated with stays, nevertheless, that no concept of the fundamental causa neurological problems and could also be hereditary. The higher eye is then used and the opposite is tion of them is essential for rational treatment. Spontaneous remedy hardly ever if ever happens in l In the primary place, faulty vision in a single eye, similar to divergent strabismus, which tends to enhance with time. Apart from the loss of binocular vision and the cosmetic l Disturbances in muscular equilibrium, normally as a result of a disfgurement, comitant squint is asymptomatic. Diplopia congenital malinsertion or faulty improvement of 1 could also be current in the preliminary levels, the history of which is or extra of the extrinsic muscular tissues, could act in the same not out there, because the onset is normally early, in small infants method, the squint being maybe preceded by a period of or very younger children, and it rapidly disappears as a result of heterophoria during which fusion was maintained. In most cases suppression is aided by an tion and convergence, a matter originally identified by actual visible defect in the eye, nevertheless it also happens in alter Donders, can also be of importance. The continuous effort of nating squint, by which each eyes have regular vision or accommodation in the hypermetrope to see clearly, even in have the same diploma of ametropia. Suppression is un the space, stimulates convergence to a higher diploma doubtedly aided, in all cases, by the peripheral state of affairs of than is compatible with binocular fxation; faced with the the picture in the squinting eye, however the important seat of sup dilemma of both stress-free his accommodation and never pression is the brain. Since the picture of any object falling seeing clearly or converging an excessive amount of and suffering diplo on disparate points ends in diplopia and since the brain pia, he chooses the latter, squints inwards and suppresses fnds this intolerable, it actively inhibits the picture of the Chapter | 26 Comitant Strabismus 417 squinting eye. It is defned as a condition with unilateral or bilateral squinting eye is used, the fovea is normally (however not invari subnormal vision (a minimum of two traces less than ‘regular’ or ably) used once more for fxation. This irregular system could two traces less than the man eye in unilateral cases) with out turn into so fxed that the fovea stays suppressed and any native ophthalmoscopic abnormality, which is reversible the eccentric retinal point could achieve prominence such that if treated appropriately at the correct time. Amblyopia com the attention could proceed to fx with the eccentric point when the monly results from situations that produce a blurred picture other eye is roofed. When the fxing eye is roofed with on the retina (amblyopia ex anopsia or stimulus deprivation the display the deviating eye normally strikes so as to take amblyopia) or cause diplopia (picture of the same object up fxation. In unilateral squints of long standing, this eye falling on disparate retinal points) or confusion (photographs of could remain motionless or move solely slightly, a condition different objects falling on the foveae of the two eyes as which is called eccentric fxation. Amblyopia happens during the critical outcome and the eyes naturally tend to return to their outdated or delicate period of improvement and maturation of the squinting place. The elimination of false correspon visible system, which is estimated to be zero–8 years in children dences is therefore of importance before operation is (zero–three years is essentially the most vulnerable period). In some cases, instead of growing eccentric blyopiogenic factors are summarized in Table 26. Single letter vision is healthier than if the letters are presented in a row as is the norm in visible acuity charts. After taking the history, the frst step in evaluating a patient this is called crowding phenomenon. Visual acuity drops less when considered by way of grey evaluation of ocular motility and common examination of neutral-density filters in comparison with regular eyes. Sometimes fxation is retained by both eye Evaluation of a Patient with Strabismus by which case the squint is said to be alternating. Usually, Case history Chief grievance in a divergent squint an object in direction of the best in the feld of vision will be fxed with the best eye, in the left Onset and duration of the feld by the left eye, whereas the converse could occur Previous treatment in convergent squint (cross-fxation). Occasionally, patients Family history with alternating strabismus can fx with both eye volun tarily, however are normally unconscious of which eye is fxing. Treatment goals and expectations the following step is to differentiate a comitant squint from an Diagnostic Visual acuity and monocular fxation sample incomitant squint. In comitant squints, when both eye is roofed after which uncovered, the deviation Determine particulars of deviation (Table 26. In acute comitant squint a patient could report diplo Management Estimate prognosis pia however the distance between the images is the same in all plan Patient/mother or father counselling instructions. Thus, in convergent squint it could be very diffcult to get the eyes to move outwards to the complete extent so Estimating the deviation: In assessing the deviation an that on maximum tried abduction of the affected eye the necessary step is to ensure that any obvious deviation is margin of the cornea may still lie inside the lateral canthus. An obvious or ‘pseudo’ squint could also be as a result of this faulty motion could also be as a result of contracture of the the confguration of the palpebral aperture. If, for example, muscle synergistic to motion of the squinting eye in the as generally happens in children, a fats nasal bridge with path of squint, for example, in a continuing left convergent epicanthus is current and the medial canthi method the squint the medial rectus of the left eye could develop contrac cornea, the appearance of a convergent squint results. This could mistakenly be diagnosed as a left lateral could show valuable in such cases. The examiner sits In incomitant squints, one should identify if it is paralytic at arm’s size in entrance of the patient and shines the beam or restrictive in nature. A easy take a look at to confrm if a defec of a direct ophthalmoscope onto the patient’s eyes. The mild tive vary of eye motion is because of muscle weak spot or a beam have to be broad enough to illuminate each eyes simulta physical restriction is the compelled duction take a look at. When the patient is orthotropic, the color and particularly the Forced Duction Test brightness of the fundus refex is equal in the two eyes. When strabismus is current, the fundus refex of the fxing It is simply an attempt to passively rotate an eyeball to its eye is darker, whereas that of the non-fxing eye is a brighter, full extent of motion to decide if the limitation of the complete lighter, purple–yellow or white colour. The difference in bright vary of eye motion is solely paralytic or whether there ness is extra necessary than the difference in colour. The take a look at is performed underneath In establishing the presence of a real deviation or squint native anaesthesia, however generally underneath common anaesthesia and further figuring out if it is latent or manifest, intermit in the case of very younger children. The patient is asked to tent or constant, alternating or unilateral, convergent or look in the path by which motion is being tested divergent, comitant or incomitant the quilt take a look at is beneficial and the utmost vary famous. The charac Interpretation: the take a look at is said to be positive if there teristics of the ocular deviation have to be determined as is a resistance to full passive motion and unfavorable if it outlined in Table 26. If one eye habitually fxes and the is feasible to passively rotate the attention absolutely with the forceps. Chapter | 26 Comitant Strabismus 419 Hirschberg take a look at No obvious squint Manifest squint Cover both eye (Cover take a look at) Cover the fixing eye (Cover take a look at) Other eye strikes to No motion Other eye stays Other eye strikes to take up fixation deviated take up fixation Blind Eccentric Immobile Pseudosquint Microtropia Intermittent squint eye fixation Remove cover Remove cover (Uncover take a look at) Squint stays momentarily after which eyes fuse or turn into straight. Cover take a look at: cover apparently fixing eye and watch motion of suspected deviating eye. Cover–uncover: take away cover above and watch motion of solely the uncovered eye, i. Alternate cover: shortly cover every eye alternately and watch the behaviour of every eye when the quilt is removed and transferred to the opposite eye. Hirschberg take a look at: shine the light of a torch on the nasion of the patient asking him/her to fixate on the light, and look ahead to symmetry of the corneal reflexes. If corrective motion is outwards, the squinting eye was convergent or esotropic. A unfavorable outcome on testing compelled duction implies a para fracture of the orbit, where each muscle entrapment and lytic or innervational squint. The anaesthetized limbus is grasped signifies a restriction as a result of contracture or fbrosis of the with a forceps and a ‘tug’ is appreciated when the patient ipsilateral antagonist or an orbital house-occupying lesion ‘makes an attempt’ to move the attention in the affected path if the stopping full motion. Force Generation Test Assessment of Binocular Vision An additional useful take a look at in immobile eyes is the active force era take a look at. Cover the apparently fixing eye with an occluder and observe the response of the opposite eye. Diagram of the place of the corneal Constant reflex as a information to the angle of the squint. Magnitude For distance and close to fxation with and with out glasses Comitancy Comitant or incomitant Hirschberg Test Laterality Unilateral A tough indication of the angle of the squint can be obtained from the place of the corneal refex when mild is thrown Alternating (which eye is preferred for fxa into the attention from a distance of about 60 cm with the ophthal tion or which eye is dominant) moscope or a targeted mild beam from a torch (Figs. The patient is asked to look at the light; an infant does convergence/ this refexly.
Diseases
Sexual disinhibition could also be a feature of frontal lobe syndromes hiv lung infection symptoms order 200 mg rebetol amex, particularly of the orbitofrontal cortex anti viral pink eye purchase rebetol with mastercard. Cross References Disinhibition; Frontal lobe syndromes; Klüver–Bucy syndrome; Punding Hypersomnolence Hypersomnolence is characterized by extreme daytime sleepiness hiv infection rates asia cheap rebetol generic, with a ten dency to hiv infected babies symptoms buy rebetol with a visa fall asleep at inappropriate occasions and places, for instance, during -187 H Hyperthermia meals, phone conversations, at the wheel of a car. Clinical signs may embody a bounding hyperdynamic circulation and sometimes papilloedema, in addition to features of any underlying neuromuscular illness. Sleep research confirm nocturnal hypoventilation with dips in arterial oxygen saturation. Cross References Asterixis; Cataplexy; Papilloedema; Paradoxical breathing; Snoring Hyperthermia Body temperature is usually regulated within slender limits via the coor dinating actions of a centre for temperature control (‘thermostat’), located in the hypothalamus (anterior–preoptic area), and effector mechanisms (shiver ing, sweating, panting, vasoconstriction, vasodilation), controlled by pathways located in or working via the posterior hypothalamus and peripherally in the autonomic nervous system. It usually implies spasticity of corticospinal (pyramidal) pathway origin, quite than (leadpipe) rigidity of extrapyramidal origin. Depending on the affected eye, this finding is often described as a ‘left-over proper’ or ‘proper-over left’. Cross References Bielschowsky’s signal, Bielschowsky’s take a look at; Cover checks; Heterotropia; Hypotropia Hypoaesthesia Hypoaesthesia (hypaesthesia, hypesthesia) is decreased sensitivity to, or diminu tion of, sensory perception in any modality, most incessantly used to describe ache (hypoalgesia) or contact. Cross Reference Anaesthesia Hypoalgesia Hypoalgesia is a decreased sensitivity to, or diminution of, ache perception in response to a usually painful stimulus. Repeated apposition of finger and thumb or foot tapping could also be useful in demonstrated hypokinesia of gradual onset (‘fatigue’). It may typically coexist with bradykinesia and hypometria and is a feature of disorders of the basal ganglia (akinetic-rigid or parkinsonian syndromes), for instance: Some variants of prion illness Cross References Akinesia; Bradykinesia; Fatigue; Parkinsonism Hypometria Hypometria is a reduction in the amplitude of voluntary movements. It could also be demonstrated by asking a patient to make repeated, large amplitude, opposition movements of thumb and forefinger, or tapping movements of the foot on the floor. Voluntary saccadic eye movements can also show a ‘step’, as a correcting additional saccade compensates for the undershoot (hypometria) of the original motion. Hypometria is a feature of parkinsonian syndromes such as idiopathic Parkinson’s illness. Cross References Akinesia; Bradykinesia; Dysmetria; Fatigue; Hypokinesia; Parkinsonism; Saccades Hypomimia Hypomimia, or amimia, is a deficit or absence of expression by gesture or mimicry. This is usually most blatant as a lack of facial expressive mobility (‘masks-like facies’). Cross References Facial paresis, Facial weak point; Fisher’s signal; Parkinsonism Hypophonia Hypophonia is a quiet voice, as in hypokinetic dysarthria. This could also be physiological, as with the diminution of the ankle jerks with normal ageing; or pathological, most usually as a feature of peripheral lesions such as radiculopathy or neuropathy. The latter could also be axonal or demyelinating, in the latter the blunting of the reflex could also be out of proportion to related weak point or sensory loss. Although incessantly characterized as a feature of the decrease motor neurone syndrome, the pathology underlying hyporeflexia may happen anywhere along the monosynaptic reflex arc, including the sensory affer ent fibre and dorsal root ganglion in addition to the motor efferent fibre, and/or the spinal twine synapse. Hyporeflexia can also accompany central lesions, particularly with involve ment of the mesencephalic and upper pontine reticular formation. Hyporeflexia is an accompaniment of hemiballismus, and can also be famous in brainstem encephalitis (Bickerstaff’s encephalitis), in which the presence of a peripheral nerve dysfunction is debated. It could also be asso ciated with many diseases, physical or psychiatric, and/or medications which affect the central nervous system. Along with hypergraphia and hyperreligiosity, hyposexuality is likely one of the defining features of the Geschwind syndrome. Cross References Hypergraphia; Hyperreligiosity Hypothermia Hypothalamic harm, particularly in the posterior area, can result in hypother mia (cf. There are many pathological causes, including tumour, trauma, infarct, haemorrhage, neurosarcoidosis, Wernicke’s encephalopathy, fats embolism, histiocytosis X, and multiple sclerosis (rare). A rare syndrome of paroxysmal or periodic hypothermia has been described and labelled as diencephalic epilepsy. Non-neurological causes of hypothermia are more common, including hypothyroidism, hypopituitarism, hypoglycaemia, and drug overdose. Cross Reference Hyperthermia Hypotonia, Hypotonus Hypotonia (hypotonus) is a diminution or lack of normal muscular tone, caus ing floppiness of the limbs. This is particularly associated with peripheral nerve or muscle pathology, in addition to lesions of the cerebellum and certain basal ganglia disorders such as hemiballismus–hemichorea. Weakness stopping vol untary activity quite than a reduction in stretch reflex activity appears to be the mechanism of hypotonia. Depending on the affected eye, this finding is often described as a ‘left-over-proper’ or ‘proper-over-left’. Cross References Cover checks; Heterotropia; Hypertropia 192 I Ice Pack Test the ice pack take a look at, or ice-on-eyes take a look at, is performed by holding an ice dice, wrapped in a towel or a surgical glove, over the levator palpebrae superioris muscle of a ptotic eye for 2–10 min. Improvement of ptosis is alleged to be spe cific for myasthenia gravis, maybe because cold improves transmission at the neuromuscular junction (myasthenic patients typically enhance in cold as opposed to hot weather). This phenomenon is mostly not noticed in different causes of ptosis, although it has been reported in Miller Fisher syndrome. A pooled anal ysis of several research gave a take a look at sensitivity of 89% and specifimetropolis of one hundred% with correspondingly excessive constructive and negative chance ratios. Whether the ice pack take a look at is also applicable to myasthenic diplopia has yet to be decided: false positives have been documented. They also happen in illness states, such as delirium, and psychiatric disorders (affective disorders, schizophrenia). Visual: illusory visual unfold, metamorphopsia, palinopsia, polyopia, teleopsia, Pulfrich phenomenon, visual alloaesthesia, visual perseveration;. They are consistent and have a compulsive quality to them, maybe triggered by the equivocal nature of the scenario. There could also be accompany ing primitive reflexes, particularly the grasp reflex, and sometimes utilization behaviour. Imitation behaviour occurs with frontal lobe harm; initially mediobasal illness was thought the anatomical correlate, but more recent research suggest upper medial and lateral frontal cortex. A distinction has been drawn between ‘naïve’ imitation behaviour, which ceases after a direct instruction from the examiner to not imitate his/her ges tures, which can be seen in some normal individuals; and ‘obstinate’ imitation behaviour which continues regardless of an instruction to stop; the latter is alleged to be unique to frontotemporal dementia. Part I: imitation and utilization behaviour: a neuropsychological study of 75 patients. Obstinate imitation behaviour in differentiation of frontotemporal dementia from Alzheimer’s illness. It is mostly seen with lesions affecting the right hemisphere, particularly central and frontal mesial regions, and may happen in affiliation with left hemiplegia, neglect, anosognosia, hemianopia, and sensory loss. Impersistence of tongue protrusion and handgrip could also be seen in Huntington’s illness. Neuropsychologically, impersistence could also be related to mechanisms of directed attention that are wanted to sustain motor activity. Neurological pathways subserving the appropriate control of micturition embody the medial frontal lobes, a micturition centre in the dorsal tegmen tum of the pons, spinal twine pathways, Onuf’s nucleus in the spinal twine segments S2–S4, the cauda equina, and the pudendal nerves. Thus, the anatomical differen tial analysis of neurological incontinence is broad. Moreover, incontinence could also be as a result of inappropriate bladder emptying or a consequence of lack of aware ness of bladder fullness with secondary overflow. Other features of the historical past and/or examination may give useful pointers as to localization. Incontinence of neurological origin is often accompanied by different neurological signs, particularly if associated with spinal twine pathology (see Myelopathy). The pontine mic turition centre lies near the medial longitudinal fasciculus and native illness may cause an internuclear ophthalmoplegia. However, different signs could also be absent in illness of the frontal lobe or cauda equina. Idiopathic generalized epilepsy with tonic–clonic seizures; nevertheless, the dif ferential analysis of ‘lack of consciousness with incontinence’ also encom passes syncopal attacks with or without secondary anoxic convulsions, non-epileptic attacks, and hyperekplexia. In addition there could also be incomplete bladder emptying, which is usually asymptomatic, as a result of detrusor sphincter dyssynergia; for publish micturition residual volumes of higher than one hundred ml (assessed by in–out catheterization or ultrasonography), that is greatest handled by clear intermittent self-catheterization.
Purchase 200 mg rebetol free shipping. Children at risk of HIV and AIDS in Moldova and Ukraine l UNICEF.
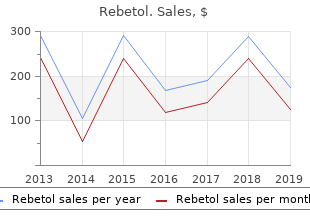
A total of 322 patients had been randomized in a 1:1:1 ratio to hiv infection pathogenesis order rebetol 200 mg amex treatment in both source hiv infection rates msm purchase rebetol overnight delivery. The median amount of Advise patients to hiv infection rates by sexuality best buy for rebetol inform their physician or pharmacist in the event that they develop any uncommon sweat manufacturing (averaged for every axilla) was 102 mg hiv infection stomach pain buy discount rebetol, 123 mg, and 114 mg for the symptoms (together with diffculty with swallowing, speaking, or respiration), or if any placebo, 50 Units and 75 Units teams respectively. Treatment responders had been defned as topics exhibiting no less than a 50% reduction from baseline in axillary sweating measured by gravimetric measurement at four weeks. If swallowing issues are severe, meals or liquids could go traces between the eyebrows (glabellar traces) in adults for a brief into your lungs. In some cases, the impact of botulinum traces in adults for a brief time frame (temporary). All emblems are the property self-catheters to empty your bladder as much as a couple of instances every day of their respective house owners. Corneal Ulceration: Diagnosis and Aggressive Treatment University of Florida Different ulcer varieties/depths Making the analysis of a corneal ulcer is important for the welfare of the affected person. In simple traumatic corneal accidents during which a small amount of epithelium is removed, healing is fast. Superficial ulceration Epithelial erosions/abrasions Recurrent "Boxer Ulcers“ Early herpes ulcers in cats – b. Perforating ulcers (Iris prolapse) Regardless of the initial cause, all ulcers are related to some iridocyclitis. Clinical indicators of ulceration: 1) Pain and blepharospasm 2) Tearing three) Purulent ocular discharge four) Miosis as a result of uveitis 5) Corneal edema/vascularization b. The major objective of present treatment methods for infectious keratitis is to sterilize the ulcer as rapidly as attainable with topically administered antibiotics. Amnion Membrane Transplants 2 “Dixie” Stacy Iris Prolapse a) Emergency b) Systemic antibiotics c) General anesthesia and surgical restore of cornea d) Topical antibiotic solutions, not ointments. Treat as simple ulcer topical antibiotics and atropine Deep, non-perforating lacerations. While considered protected and effective, their use has been rarely difficult by the event of antibodies that cut back or negate their therapeutic impact. The presence of antibodies has been attributed to shorter dosing intervals (and booster injections), greater doses per injection cycle, and better quantities of antigenic protein. Some newer formulations with purified core neurotoxin devoid of accessory proteins could have decrease general immunogenicity. Keywords: botulinum toxin; immunogenicity; immunoresistance; bioassays; medical resistance testing; neutralizing antibodies Key Contribution: this review highlights the background of immunogenicity in botulinum toxin treatment, discussing its prevalence, detection, and administration, as well as widespread pitfalls. In 324 people who acquired a subsequent booster dose, antibodies had been detectable in ninety nine% after 24–36 days [6]. Titers probably can also remain elevated in patients with earlier botulism publicity [7]. The onabotulinumtoxinA (Botox) package deal insert recommends storage of the 100 unit vials as much as 36 months at 2 ◦C to 8 ◦C [8]. When reconstituted and refrigerated, efficiency loss begins at 12 h, and ends in a 69. These pseudo non-responsive disorders are more prevalent than true immune-mediated major non-responsiveness. Other patients could have situations which might be recognized to be difficult to deal with, similar to pre-existing anterocollis (as famous above), or contractures because of lengthy-standing abnormal posture. There can be a discordance between affected person and provider perceptions of benefit [17]. This is largely driven by affected person observations that benefits of injections frequently final lower than three months and, therefore, many patients would prefer shorter inter-dose intervals to keep efficacy. In one study of 30 patients with a wide range of dystonias who acquired shorter intervals of incobotulinumtoxinA dosing, with a mean 9. The core neurotoxin consists of a 150 kD inactive precursor protein that incorporates a 100 kD heavy chain and 50 kD gentle chain, linked by a disulfide bond [29]. The impaired Ach exocytosis interferes with synaptic neural transmission in striate muscle tissue as well as different cholinergically innervated constructions, similar to easy muscle tissue or exocrine glands, together with salivary glands [24]. DaxibotulinumtoxinA, a brand new formulation at present in development has a singular peptide excipient (described further below) [34]. This peptide is presumably designed to cut back diffusion of the neurotoxin and consequently increase its period of impact. A related extended impact was famous in another section 2 trial analyzing its use in the treatment of glabellar traces [39]. These findings, nevertheless, must be confirmed by larger, section three studies which might be at present being performed in a number of facilities. This is supported by a relatively low frequency of antibody formation in patients handled with incobotulinumtoxinA [19,24,51]. Inactive protein refers to the 150 kD precursor protein formed prior to further protease cleaving right into a 100 kD heavy chain and 50 kD gentle chain. Although Toxins 2019, eleven, 491 6 of twenty-two inactive, this 150 kD protein bears the identical epitopes because the heavy and lightweight chain and remains immunogenic [52]. Consequently, products with the next ratio of inactive to energetic toxin are more susceptible to generating antibodies and have a decrease specific biological activity, which denotes the ratio of biologic activity to antigenic toxin [53]. Historically, the most notable instance of product property affecting antigenicity is the transition from the unique formulation of onabotulinumtoxinA to the newer formulation of onabotulinumtoxinA in 1997 [7]. Antibody formation was discovered to be six instances more doubtless with the unique formulation than with the newer formulation [fifty four]. Characteristics of the patients themselves can also have an effect on rates of immunogenicity. Various laboratory assays have been used to detect antibodies in patients with attainable immunoresistance (Table 1). In this assay, a affected person’s serum is incubated with a standardized quantity of neurotoxin, and this neurotoxin is delivered through intraperitoneal injection into several mice. Some studies have used a qualitative version of this assay, where four mice are injected with the serum/neurotoxin combination, and a constructive Ab outcomes denotes the survival of three mice [fifty eight]. In another meta-evaluation of patients handled with the decrease protein formulation of onabotulinumtoxinA, eleven/2240 (zero. However, seven of these eleven patients continued to have medical response, however two of these seven had only a transiently constructive test. Clinical responsiveness, nevertheless, is usually difficult to define, notably when just one or two medical evaluations are available, because of the placebo response and different components. The assay, though costly, is still commercially out there at pacificbiolabs. In this test, the left hemidiaphragm and phrenic nerve of a mouse are excised and placed in an organ bathtub. A serum/neurotoxin combination is utilized to the assay, and the time to attain half-most of an electrically induced twitch drive is measured. Although the assay is meant to detect blocking antibodies, the authors famous that their patients had been “still responding. Varying sensitivities and specificities had been famous with different antigen coating concentrations and serum dilutions. The one affected person with discrepant outcomes was famous to have a borderline medical response. Legend: By conference the following are injected into the right medial eyebrow: 20 U of onabotulinumtoxinA; incobotulinumtoxinA, 50 U dosages are injected into the right medial eyebrow: 20 U of onabotulinumtoxinA; of abobotulinumtoxinA, or 1000 U of rimabotulinumtoxinB. In one study, 20 patients assessment for asymmetry of forehead wrinkling on eyebrow elevation [fifty nine]. Reduction percentages which might be two commonplace deviations below a beforehand measured mean reduction in a control group are considered abnormal. In this test, the affected person is dropped at a room with managed temperature and humidity, and presses their palm on a paper, which is then dyed and fixed with a 1% ninhydrin resolution. Nevertheless, some consistent patterns have emerged from the review of the literature. In patients handled with the unique onabotulinumtoxinA formulation for blepharospasm, these receiving <500 items/year had a four% prevalence of antibodies, whereas these receiving >500 items/year had a sixty three% prevalence of antibodies [7]. In a meta-evaluation together with four studies analyzing onabotulinumtoxinA in spasticity, only 1/317 patients (zero. In another study of 279 patients receiving lengthy-term treatment of higher limb spasticity with onabotulinumtoxinA, only certainly one of 224 examined patients ( Mimosa farnesiana (Cassie Absolute). Rebetol. Source: http://www.rxlist.com/script/main/art.asp?articlekey=96607
Raleigh Office:
5510 Six Forks Road
Suite 260
Raleigh, NC 27609
Phone
919.571.0883
Email
info@jrwassoc.com
© 2017 JRW Associates. All Rights Reserved


